


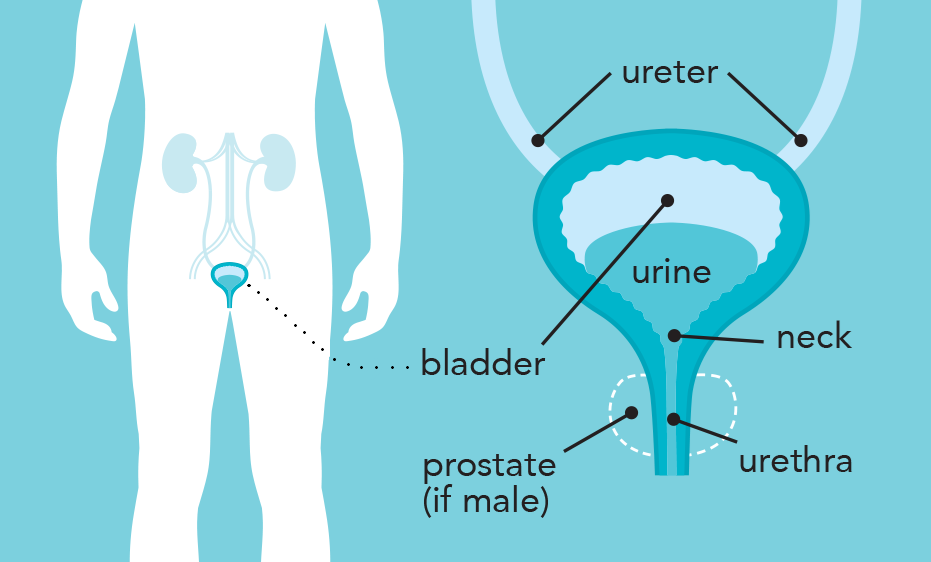
Bladder cancer develops when abnormal cells in the lining of the bladder (called the urothelium) begin to grow and divide in an uncontrolled way. Over time, these abnormal cells can form a lump or mass which can develop into cancer. The cancer may grow into deeper layers of the bladder wall or, in some cases, spread to other parts of the body.

The most common type of bladder cancer is urothelial carcinoma (also called transitional cell carcinoma), accounting for around 90% of cases. It starts in the urothelial cells that line the inside of the bladder.
Less common types of bladder cancer include squamous cell carcinoma (~2% of cases), which develops from thin, flat cells in the bladder lining, and adenocarcinoma (~1% of cases) which starts in mucus producing gland cells within the bladder.
Bladder cancer can be described based on how far the cancer has grown or spread:
- Non muscle invasive bladder cancer (NMIBC)
The cancer is limited to the inner lining of the bladder (the urothelium) and the layer just beneath it (the lamina propria). It has not spread into the muscle layer of the bladder wall. Around 75% of people with bladder cancer are diagnosed at this early stage. NMIBC is further classified into low , intermediate , and high risk groups based on features such as tumour grade and stage (see How is bladder cancer diagnosed?), which helps guide treatment and follow up. - Muscle invasive bladder cancer (MIBC)
The cancer has spread into the muscle layer of the bladder wall. In some cases, it may also have started to spread through the bladder wall or to nearby tissues or lymph nodes. - Advanced or metastatic bladder cancer
The cancer has spread outside of the bladder and may have spread to distant lymph nodes or other parts of the body, such as the lungs, liver, or bones. This is known as metastatic disease.
The following sections will focus on urothelial carcinoma.
The exact cause of bladder cancer is largely unknown. However, research shows that people with certain risk factors are more likely to develop bladder cancer.
These risk factors include:
- Smoking (the strongest known risk factor)
- Older age
- Being male
- Work exposure to certain chemicals (called aromatic amines). These chemicals are used in some jobs, such as making rubber, plastics, and dyes. Long-term workplace exposure to these chemicals can increase the risk of bladder cancer.
- Previous radiation therapy to the lower abdomen or pelvis
- Family history of bladder cancer and some genetic conditions
- Use of certain medicines, such as the chemotherapy drug cyclophosphamide
Having one or more risk factors does not mean a person will develop bladder cancer. Many people with risk factors never develop cancer, and some people are diagnosed without any known risk factors.
If you have concerns about your risk factors or health, talk to your doctor or specialist.
Sometimes bladder cancer causes few or no symptoms and is found when a urine test is done for another reason. However, most people do notice symptoms.
Symptoms may include:
- Blood in the urine (haematuria)
This is the most common symptom of bladder cancer. It may appear suddenly or come and go and is usually not painful. The urine may look pink, red, or brown. - Changes in bladder habits, such as:
- pain or a burning sensation when urinating
- needing to urinate more often
- a strong or urgent need to pass urine
- difficulty emptying the bladder
- Pain in the lower abdomen (tummy) or back
- Unexplained weight loss (less common)
Not everyone with these symptoms has bladder cancer, but if you have any of these symptoms, or if you are concerned about your health, it is important to see your doctor.
Never ignore blood in your urine. If you see blood, contact your doctor as soon as possible.
If you have symptoms that may suggest bladder cancer, you will usually see your general practitioner (GP) first. Your GP may arrange some initial tests and, if needed, refer you to a specialist for further investigation.
The following tests may be recommended to confirm the diagnosis and plan treatment:
General health tests
- Physical examination, which may include an internal examination
- Blood and urine tests, including urine tests to check for blood or abnormal cells
Main tests
- Cystoscopy
This is the main test used to diagnose bladder cancer. A thin tube with a light and camera on the end (a cystoscope) is passed through the urethra to look directly at the bladder lining. It may be done under local or general anaesthetic and can use a flexible or rigid scope. - Biopsies or transurethral resection of bladder tumour (TURBT)
During a cystoscopy, your doctor may take small samples from the lining of the bladder (called biopsies). If an abnormal area is found, it may be removed at the same time in a procedure called a transurethral resection of bladder tumour (TURBT). The tissue is then sent to a laboratory to be checked under a microscope. This helps confirm whether cancer is present, what type it is, and how far it has grown into the bladder wall.
Imaging tests
Other imaging tests may be recommended to show how far the cancer has grown or whether it has spread to other parts of the body. These may include:
- CT (computed tomography) scan
Uses X-rays and a computer to create detailed pictures of the bladder, nearby lymph nodes, and other parts of the body. A contrast dye injected into a vein may be used to help highlight abnormal areas. - MRI (magnetic resonance imaging) scan
Uses a strong magnet and radio waves to produce detailed cross-sectional images. An MRI can help show how deeply the cancer has grown into the bladder wall. A contrast dye injected into a vein may be used to help highlight abnormal areas.
Other tests may include:
- Ultrasound
A handheld device (transducer) is moved over the abdomen (tummy). High-frequency sound waves create pictures of the bladder and nearby organs. - PET (positron emission tomography)-CT scan
A scan that uses a small amount of radioactive liquid to highlight areas of increased activity in the body, which may be a sign of cancer. - Bone scans or x-rays may also be recommended
The results of these tests help doctors understand how far the bladder cancer has spread in the body (this is called the stage) and how abnormal the cancer cells look under the microscope and how likely they are to grow or spread (the grade). This information helps guide decisions about the most appropriate treatment.
Staging bladder cancer
Doctors may use the TNM staging system to describe the cancer stage:
- T (Tumour) – describes the size of the tumour and how far it has grown within the bladder or into nearby structures (Ta, Tis, T1–T4)
- N (Nodes) – whether the cancer has spread to nearby lymph nodes
- N0: no spread to lymph nodes
- N1-N3: spread to nearby lymph nodes
- M (Metastasis) – whether the cancer has spread to distant parts of the body
- M0: no distant spread
- M1: distant spread present
The TNM results are often put together to give an overall stage of bladder cancer, ranging from Stage 0 (earliest stage) to Stage IV (most advanced stage).
Grading bladder cancer
Grading is done by examining cancer cells under a microscope, usually from a biopsy or after surgery. The grade describes how abnormal the cancer cells look compared with normal bladder cells. It gives an idea of how quickly the cancer may grow.
- Low-grade cancers – the cancer cells look similar to normal bladder cells and are usually slow-growing
- High-grade cancers – the cancer cells look very abnormal and tend to grow more rapidly. They are more likely to spread into the bladder muscle and outside the bladder.
Superficial (non-muscle invasive) bladder cancers can be either low-grade or high-grade. In contrast, muscle-invasive bladder cancers are typically high-grade.
Risk category
Superficial (non-muscle-invasive) bladder cancers may also be classified as having a lower or higher risk of coming back after treatment or spreading into the muscle layer. This risk assessment is based on factors such as the cancer’s stage, grade, and other features.
- Type and stage of bladder cancer
- Whether you have symptoms
- Your overall health, and
- Your preferences
It is important to take time to discuss your treatment options, including possible benefits and side effects, with your doctor before deciding which treatment is right for you.
Treatment options may include one or more of the following:
Surgery:
- TURBT
Many early-stage bladder cancers are treated with surgery called transurethral resection of bladder tumour (TURBT), where the cancer is removed through the urethra without making an incision in the abdomen. This is usually done under general anaesthetic. - Radical cystectomy and urinary diversion
For some people with high-risk non-muscle-invasive bladder cancer or muscle-invasive bladder cancer, surgery to remove the entire bladder and nearby lymph nodes (called a radical cystectomy) may be recommended. After the bladder is removed, surgeons create a new way for urine to leave the body. This is called a urinary diversion. Options may include:- neobladder, where a new bladder is made using part of the bowel
- urostomy, where urine drains into a bag on the outside of the abdomen
Your surgeon will discuss the most suitable option with you.
Chemotherapy
Chemotherapy uses drugs to damage or kill rapidly dividing cells, such as cancer cells.
Chemotherapy can be given in two main ways in bladder cancer:
- Directly into the bladder (called intravesical treatment) through a tube (catheter) inserted into the urethra. Intravesical treatment may be used for non-muscle-invasive bladder cancer, usually after TURBT surgery, to help reduce the risk of the cancer coming back.
- Through a drip into a vein (intravenously), so it can travel through the whole body (this is called systemic chemotherapy). This may be given before or after surgery (radical cystectomy), or as the main treatment for advanced or metastatic bladder cancer. It is often given as a combination of drugs and may be used alongside other treatments, such as immunotherapy.
Immunotherapy
Immunotherapy helps the body’s immune system to attack and destroy cancer cells.
- BCG (Bacillus Calmette–Guérin)
BCG (Bacillus Calmette–Guérin) is a vaccine-based treatment used to treat early-stage bladder cancer. It is given directly into the bladder (intravesical BCG) through a thin tube passed into the bladder via the urethra. BCG works by activating the immune system in the bladder to help fight cancer cells and reduce the risk of bladder cancer coming back or becoming more invasive. Checkpoint inhibitors
Checkpoint inhibitors are a type of immunotherapy that help the body’s immune system recognise and attack cancer cells. They may be used before or after surgery (radical cystectomy) in some people, or as the main treatment for advanced or metastatic bladder cancer. They may be given alone or together with other treatments, such as chemotherapy. These medicines are usually given through a drip into a vein (intravenously).
How do checkpoint inhibitors work? T cells are a type of immune cell and are part of the body’s natural defence system. They help the body recognise and destroy abnormal cells. T cells have built-in “checkpoints” that act like brakes, helping prevent them from attacking healthy cells. Some cancer cells use these checkpoints to avoid being detected by the immune system. Checkpoint inhibitors are medicines that block these checkpoints, allowing T cells to better recognise and attack cancer cells.
Radiation therapy (radiotherapy)
Radiation therapy uses high-energy radiation to damage and kill cancer cells. It may be used on its own or in combination with other treatments, such as chemotherapy.
Antibody drug conjugates
Antibody–drug conjugates (ADCs) are a type of targeted cancer treatment used in advanced or metastatic bladder cancer. ADCs are usually given through a drip into a vein (intravenously).
ADCs are made up of two main parts:
- An antibody, which is designed to find and attach to specific markers on cancer cells.
- A chemotherapy drug, which is linked to the antibody.
The antibody acts like a guide, carrying the chemotherapy directly to the cancer cells. Once attached, the chemotherapy is released inside the cancer cell to kill or damage it.
Note: Antibody–drug conjugates are not currently widely used as standard treatment for bladder cancer in New Zealand. Access may be limited, and they may be available in certain circumstances, such as through clinical trials or specialist care.
Clinical trials
For general information about clinical trials, please click here: What is a clinical trial?
For information about ANZUP bladder cancer trials click here: Bladder cancer trials
All treatments can have side effects, which vary from person to person. Your doctor will discuss the possible benefits and risks with you.
Complementary and alternative therapies
- Complementary therapies are designed to be used alongside conventional medical treatment and may be used to help manage side effects of cancer or its treatment. They may include massage, psychological techniques or herbal medicines.
- Alternative therapies are used instead of conventional medical treatment. Most have not been scientifically tested for safety or effectiveness, and some therapies may interfere with cancer treatments or cause harm.
It is important to tell your cancer doctor about any complementary or alternative therapies you are using or considering before starting or during cancer treatment.