

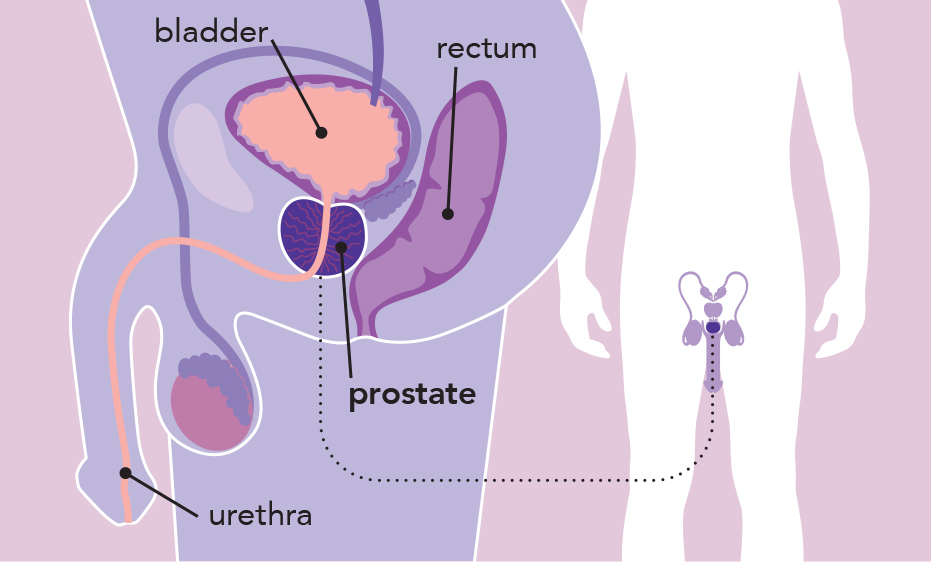
What is prostate cancer?
Prostate cancer develops when abnormal cells in the prostate begin to grow and divide in an uncontrolled way. Over time, these cells may form a lump or mass which can develop into a cancer, which can grow into nearby tissues or spread to other parts of the body.

There are several types of prostate cancer. However, the vast majority (around 96%) are adenocarcinomas, which develop in the cells that make prostate fluid, a component of semen. While many of these cancers grow slowly and are unlikely to spread beyond the prostate, some can grow and spread more rapidly.
Prostate adenocarcinoma is usually described based on how far it has spread:
- Localised (early) prostate cancer
The cancer is contained within the prostate and has not spread anywhere else in the body.
- Locally advanced prostate cancer
The cancer has spread outside the prostate into nearby tissues or organs, such as the pelvic lymph nodes, bladder, or lower bowel (rectum), but has not spread to distant parts of the body.
- Advanced or metastatic prostate cancer
The cancer has spread beyond the pelvis (lower abdomen) to distant parts of the body, most commonly to lymph nodes or to the bones. This is known as metastatic disease.
Prostate cancer is further described as low-risk, intermediate-risk, or high-risk, based on factors such as the PSA level, cancer grade (Gleason score or ISUP grade group), and the extent of cancer found on biopsy. (See Glossary)
Less commonly, other types of cancer can develop in the prostate, such as sarcomas, small cell carcinoma, or neuroendocrine tumours. These rarer types often behave differently from the more common prostate adenocarcinoma.
The following sections focus on prostate adenocarcinoma.
What are the risk factors for prostate cancer?
Anyone with a prostate can develop prostate cancer. Although the exact cause is largely unknown, research shows that people with certain risk factors are more likely to develop prostate cancer.
These include:
- Age: The risk of prostate cancer increases with age. It is uncommon in men under 50, with most cases diagnosed in older people.
- Family history: Having a father or brother who has had prostate cancer, especially if diagnosed at a younger age (such as before age 60), increases the risk.
- Genetic factors: An increased risk is seen in people with a strong family history of breast or ovarian cancer, particularly when linked to inherited gene changes such as BRCA1 or BRCA2.
- Ancestry: People of African ancestry may have a higher risk of developing prostate cancer and may be more likely to be diagnosed at a later stage or with more advanced disease.
Having one or more risk factors does not mean a person will develop prostate cancer. Many people with risk factors never develop cancer, and some people are diagnosed without any known risk factors.
If you have concerns about your risk factors or health, talk to your doctor or specialist.
What are the symptoms of prostate cancer?
Early prostate cancer often causes no symptoms, or only mild changes in urination that may be easy to overlook or attribute to ageing. Even advanced prostate cancer may not cause noticeable symptoms in some people.
When symptoms do occur, they may include:
- Needing to urinate more often, during the day and/or night
- Feeling a sudden, urgent need to urinate
- Difficulty starting urination, a weak urine flow, or urine flow that stops and starts
- A feeling that the bladder is not completely empty after passing urine
- Discomfort or pain when urinating
- Blood in the urine or semen
- Erection problems
- Unexplained weight loss
- Bone pain – such as in the lower back, hips, pelvis, upper thighs, or spine — which may indicate the cancer has spread beyond the prostate
Some of these symptoms can also be caused by non-cancerous conditions, such as benign prostatic hyperplasia (BPH), which is a normal enlargement of the prostate with age.
If you notice any symptoms or have concerns about your health, it is important to talk to your doctor.
Prostate cancer is often easier to treat when it is diagnosed early.
How is prostate cancer diagnosed?
Your doctor may arrange some initial tests. If needed, you will be referred to a specialist (usually a urologist) for further investigation.
Some of the following tests may be recommended to confirm the diagnosis and plan treatment:
General health and blood tests
- A general physical examination
- Blood tests, including a prostate-specific antigen (PSA) test, which measures a protein made by the prostate.
Note: A high PSA test result does not always mean prostate cancer. PSA levels can also be raised by other factors, such as age, prostate size, urinary or prostate infections, ethnicity, and some medications.
- Urine tests
Digital rectal examination (DRE)
- The doctor (usually the urologist) gently inserts a gloved, lubricated finger into the rectum (back passage) to feel the size, shape and firmness of the prostate.
MRI (magnetic resonance imaging) scan
- An MRI uses magnets and radio waves to produce detailed cross-sectional images of inside the body
- A specialised MRI called multiparametric MRI (mpMRI) may be used to assess the size of the prostate and identify areas that may be suspicious for cancer
- A contrast dye injected into a vein may be used to help highlight abnormal areas
Biopsy
- A biopsy is a procedure where multiple small samples of tissue are taken from the prostate using a thin needle. The procedure is done using local or general anaesthesia. There are two main ways a prostate biopsy can be performed:
- Transperineal: the needle is inserted through the skin between the anus and scrotum
- Transrectal: the needle is inserted into the prostate through the rectum (back passage)
Your urologist will discuss the most suitable option and explain the risks and benefits.
- The biopsy samples are sent to a laboratory, where a specialist doctor, called a pathologist, looks at them under a microscope. This helps confirm whether cancer is present, what type of prostate cancer it is, and features such as the grade, which gives an indication of how quickly the cancer is likely to grow.
Other imaging tests
If prostate cancer is confirmed, other imaging tests may be recommended to help show how far the cancer has grown or spread in the body (the stage). These may include:
- PSMA PET/CT (positron emission tomography/computed tomography) scan
A PSMA PET/CT scan is a special scan used to look for prostate cancer in the body. A small amount of a radioactive material (known as a tracer) is injected into a vein. This tracer attaches to a protein called prostate-specific membrane antigen (PSMA), which is commonly found on the surface of prostate cancer cells. The PET scanner detects areas with higher levels of the radioactive tracer and shows where prostate cancer cells are located, both in the prostate and in other parts of the body, such as the lymph nodes or bones.
- CT (computed tomography) scan
Uses X-rays and a computer to create detailed images of the prostate, lymph nodes, and other parts of the body. A contrast dye injected into a vein may be used to show abnormal areas more clearly.
- Bone scan
May be used to check whether cancer has spread to the bones
The results of these tests help doctors understand how far the prostate cancer has spread in the body (this is called the stage) and how the cancer cells look under the microscope and how likely they are to grow or spread (this is called the grade). This information helps doctors plan the most appropriate treatment.
Staging
Doctors may use the TNM staging system to describe the stage of prostate cancer.
| TNM staging system | |
| T stands for tumour | Refers to the size of the tumour (T0–4). T0 is smaller and T4 is larger. |
| N stands for nodes | N0 means the cancer has not spread to lymph nodes; N1 means it has spread to lymph nodes in the pelvis. |
| M stands for metastasis | M0 means the cancer has not spread outside of the pelvis; M1 means it has spread to lymph nodes, bone or other organs outside the pelvis. |
The TNM results are often put together to give an overall stage of prostate cancer, ranging from Stage I (earliest) to Stage IV (most advanced).
Grading and grading systems
Grading is determined by examining cancer cells under a microscope after a biopsy. The more abnormal the cells appear compared to normal prostate cells, the higher the grade and generally, the more aggressive the cancer.
- Low-grade cancers: cancer cells look similar to normal prostate cells and are usually slow-growing.
- High-grade cancers: cancer cells look very abnormal and tend to grow more quickly.
Doctors use grading systems to describe the grade of prostate cancer and help guide treatment decisions. The most commonly used grading systems are:
- Gleason score – ranges from 6 to 10 with a higher score indicating a more aggressive cancer
- ISUP Grade Group – ranges from Grade Group 1 to 5 with a higher grade group also indicating a more aggressive disease
Genetic and genomic testing
For people with advanced (metastatic) prostate cancer, or a strong family history of cancers such as prostate, breast, ovarian or pancreatic cancer, genetic or genomic testing may be discussed. This discussion may include referral to a genetic counsellor or a familial cancer clinic. Although the names sound similar, these two tests look for different things:
- Genetic testing: “was I born with this?” This usually involves a blood or saliva (spit) sample. It looks for inherited changes (mutations) in genes such as BRCA1 or BRCA2.
- Genomic testing: “what has changed in my cancer?” This looks for changes (mutations) that have developed in the prostate cancer cells themselves. These are not inherited and cannot be passed on to family members. This testing is usually done on a tumour sample, such as tissue taken during a biopsy or surgery.
- The results of genetic or genomic testing may help guide treatment options. Genetic testing results may also help identify cancer risk for family members.
How is prostate cancer treated?
If prostate cancer is diagnosed, your doctor may discuss your case with other health professionals at a multidisciplinary team (MDT) meeting. This team may include urologists, medical oncologists, radiation oncologists, nurses, and allied health professionals such as physiotherapists. The MDT works together to recommend the most appropriate treatment options for you.
Treatment recommendations for prostate cancer depend on several factors, including:
- The type and stage of prostate cancer
- If the cancer is localised (contained within the prostate), whether it is low-, intermediate- or high-risk
- If the cancer has spread beyond the prostate to other parts of the body (metastasised)
- Whether you have had previous treatment for prostate cancer, including the type of treatment
- Your overall health and any other medical conditions
- Your personal preferences
It’s important to take time to talk with your doctor about your treatment options, including the possible benefits and side effects, before deciding what’s right for you.
Treatment may include one or more of the following options, depending on individual circumstances:
Active surveillance and watchful waiting
- Active surveillance
Active surveillance involves closely monitoring prostate cancer with regular, planned check-ups rather than starting treatment straight away. Monitoring usually includes regular PSA blood tests, digital rectal examinations, imaging tests such as MRI scans, and sometimes repeat biopsies.
If monitoring tests show that the cancer is starting to grow or change, active treatment, such as surgery or radiation therapy, may be recommended.Active surveillance may be an option for people with low-risk (and sometimes intermediate-risk) localised prostate cancer (contained within the prostate) that is not causing symptoms.
- Watchful waiting
Watchful waiting also involves monitoring prostate cancer without starting treatment straight away. However, it usually entails fewer tests than active surveillance.
Treatment is generally only considered if symptoms develop and need to be managed. The main goal of watchful waiting is to maintain quality of life, rather than to cure the cancer.Watchful waiting may be suitable for people with localised, locally advanced, and sometimes advanced, prostate cancer who are not suitable for active treatment because of other health conditions and/or a shorter life expectancy.
Surgery (radical prostatectomy)
Surgery for prostate cancer is called a radical prostatectomy. It involves removing the prostate, the seminal vesicles, and a short section of the urethra (the tube that carries urine from the bladder to the penis). After the prostate is removed, the urethra is rejoined to the bladder. The vas deferens, which carry sperm from the testicles, are cut and sealed. In some cases, nearby pelvic lymph nodes may also be removed or biopsied.
Surgery can be performed using an open approach, laparoscopic (keyhole) surgery, or robotic-assisted surgery. Each approach has potential benefits and risks, which should be discussed with your surgeon.
Surgery may be an option for people with localised and locally advanced prostate cancer. In some cases, surgery may also be combined with other treatments, such as hormonal or radiation therapy.
Radiation therapy (radiotherapy)
Radiation therapy uses high-energy radiation to damage cancer cells and stop them from growing. It may be delivered in different ways:
- External beam radiation therapy (EBRT):
Radiation is delivered to the prostate or other treatment areas by a machine outside the body, usually over a number of treatment sessions.
- Brachytherapy:
Involves placing radioactive seeds directly into or near the prostate cancer
Radiation therapy may be used to treat localised or locally advanced prostate cancer, either on its own or in combination with other treatments such as hormone therapy or surgery. It may also be used in advanced or metastatic prostate cancer to help control cancer growth and relieve symptoms.
Hormone (blocking) therapy or androgen targeted therapy
Androgens, such as testosterone and dihydrotestosterone (DHT), are hormones produced naturally in the body to help build muscle, maintain bone strength, and support sexual function. In prostate cancer, these hormones can help drive the growth and spread of cancer cells. Androgen-targeted (hormone) therapy works by lowering androgen levels or blocking their effects on prostate cancer cells. This can shrink or slow the growth of prostate cancer. For some men, this effect can last many years, while for others the cancer may become less responsive to treatment sooner.
There are several types of hormone therapy used to treat prostate cancer which work in different ways.
- Treatment to lower testicular androgen levels
This type of hormone therapy lowers the amount of testosterone made by the testicles and is often called androgen deprivation therapy (ADT). It forms the basis of most hormone treatments for prostate cancer. ADT is commonly given as medicines called gonadotrophin-releasing hormone (GnRH) agonists or antagonists, which are usually administered as regular injections or as small implants placed under the skin by your GP, specialist or nurse. These medicines work by reducing or stopping the body’s production of testosterone.
This type of ADT may be used to treat localised, locally advanced, or advanced (metastatic) prostate cancer. It can be used on its own or alongside other treatments such as radiation therapy, chemotherapy, surgery, or other hormone therapies.
Less commonly, ADT may involve surgery to remove the testicles (orchidectomy).
- Drugs that stop androgens from working
Anti-androgens block the action of testosterone on prostate cancer cells, preventing it from stimulating cancer growth.
Anti-androgens are taken as tablets and are usually used in combination with ADT, and sometimes alongside other anti-cancer treatments. These medications are referred to as androgen receptor pathway inhibitors (ARPIs).
- Treatment to lower androgen levels from other parts of the body
Even when ADT is used to reduce androgen production in the testicles, small amounts of male hormones can still be produced by other parts of the body, such as the adrenal glands and the prostate cancer cells themselves.
CYP17 inhibitors () reduce androgen production in these other parts of the body by blocking an enzyme needed to make male hormones. They are taken as tablets and are usually prescribed with a low dose of steroid to replace the body’s natural steroid levels that may be reduced by these medications and to help reduce side effects.
CYP17 inhibitors are typically used in combination with ADT, and sometimes with other treatments.
Chemotherapy
Chemotherapy uses medicines to damage or kill rapidly dividing cells, such as cancer cells. In prostate cancer, chemotherapy is usually given through a drip into a vein (intravenously).
Chemotherapy may be offered as part of combination treatment for advanced or metastatic prostate cancer, or to treat prostate cancer that no longer responds to hormone therapy.
Other treatments
- Radioligand therapy
Radioligand therapies, such as lutetium-177 PSMA, involve injecting a radioactive medicine into the bloodstream. This medicine is designed to attach to a protein called PSMA (Prostate-Specific Membrane Antigen), which is commonly found on prostate cancer cells. Once attached, the medicine delivers radiation directly to the cancer cells, helping to damage or destroy them. Because the treatment travels through the bloodstream, it can reach and treat prostate cancer throughout the body.
- Please note: Lutetium-177 PSMA therapy is not currently approved (registered) by Medsafe in New Zealand This means it is not part of standard treatment, although it may still be available in certain circumstances, such as through clinical trials or specialist care.
- Targeted therapy: PARP (poly [ADP-ribose] polymerase) inhibitors
PARP inhibitors are a type of targeted treatment used for some people with prostate cancer, particularly those with certain genetic changes such as BRCA1 or BRCA2. Cancer cells with a BRCA mutation are already missing one of their key DNA repair systems. . PARP inhibitors block another DNA repair pathway that these cancer cells rely on, so they can no longer repair themselves and may die. These treatments are taken as tablets.
Clinical trials
For general information about clinical trials, please click here: What is a clinical trial?
For information about ANZUP prostate cancer trials click here: Prostate cancer trials
All treatments can have side effects, which vary from person to person. Your doctor will discuss the possible benefits and risks with you.
Complementary and alternative therapies
- Complementary therapies are used alongside conventional medical treatment and may help manage symptoms or side effects of cancer or its treatment. These may include massage, psychological or relaxation techniques, and some herbal or natural therapies.
- Alternative therapies are used instead of conventional medical treatment. Most have not been scientifically tested for safety or effectiveness, and some therapies may interfere with cancer treatments or cause harm.
It is important to tell your cancer doctor about any complementary or alternative therapies you are using or considering before starting or during cancer treatment.

