

Penile cancer starts when abnormal cells in the skin of the penis begin to grow and divide in an uncontrolled way. Over time, these cells can form a lump (tumour) or an open sore (ulcer) which can develop into cancer.

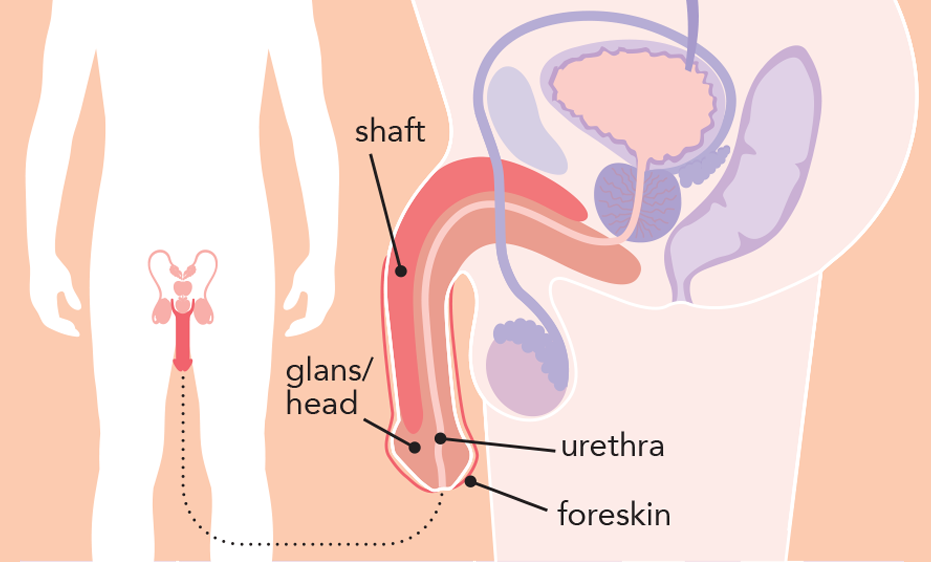
Penile cancer can start on the foreskin, the shaft (body), or the head of the penis (glans).
Penile cancer can affect anyone with a penis, but it is most diagnosed in men over the age of 50. Most penile cancers start in the surface layer of the skin of the penis, called the epithelium.
The most common type is squamous cell carcinoma (SCC), which accounts for about 95% of penile cancers. SCC starts in flat skin cells called squamous cells. It most often develops on the inner foreskin (in people who are not circumcised) or on the head of the penis (glans), but it can also occur on the shaft (body) of the penis.
Carcinoma in situ (CIS), also known as penile intraepithelial neoplasia (PeIN), is an early form of squamous cell cancer. In this condition, abnormal cells are found only in the top layer of the skin and have not spread deeper. CIS is considered a precancerous condition, as it can develop into invasive cancer over time.
Other much less common types of penile cancer include:
- Basal cell carcinoma, which usually grows slowly and starts in deeper layers of the skin
- Adenocarcinoma, which develops from sweat glands in the penis
- Melanoma of the penis, which starts in pigment producing cells that give skin its colour
- Penile sarcoma, which develops in deeper tissues such as blood vessels, muscle, or fat and is very rare
Penile cancer is rare and the cause remains unknown. However, research shows that people with certain risk factors have a higher chance of developing penile cancer.
These risk factors include:
- Human papillomavirus (HPV) infection
HPV is a common group of viruses spread through sexual contact. Some types of HPV increase the risk of certain cancers. Most people with HPV do not develop cancer, but HPV is found in around half of all penile cancers. - Not being circumcised
- Phimosis: a condition where the foreskin is too tight to pull back. This can make cleaning difficult and may lead to ongoing irritation, inflammation, or infection.
- Smoking
- Increasing age. Penile cancer is more common in people aged over 50.
- Certain long-term skin conditions, such as lichen sclerosus or psoriasis
- Human immunodeficiency virus (HIV) infection or acquired immunodeficiency syndrome (AIDS)
- Untreated precancerous conditions, such as carcinoma in situ
- Long-term exposure to ultraviolet (UV) light, including sunlight or UV lamps
Having one or more risk factors does not mean you will develop penile cancer. Many people with risk factors never develop cancer, and some people develop penile cancer without any known risk factors.
If you have concerns about your risk factors or health, talk to your doctor or specialist.
Early symptoms of penile cancer may include:
- a sore, growth, or ulcer on the head of the penis (glans), the foreskin, or the shaft (body) of the penis that does not heal within a couple of weeks
- bleeding from the penis or from under the foreskin
- a smelly or unusual discharge under the foreskin
- a firm or hard lump on or under the foreskin
- thickening of the skin on the penis or foreskin, which may make it difficult to pull back the foreskin
- changes in skin colour on the penis or foreskin
- pain or discomfort in the shaft or tip of the penis
- swelling at the tip of the penis
- a rash or persistent red patch on the penis that does not go away
- lumps under the skin in the groin, which may be due to swollen lymph nodes
These symptoms can also be caused by other, less serious conditions. However, it is important to see your doctor if you notice any new or ongoing changes.
Penile cancer is usually easier to treat when diagnosed early.
If you have symptoms that may suggest penile cancer, you will usually see your general practitioner (GP) first. Your GP may arrange some initial tests and, if needed, refer you to a specialist (usually a urologist) for further investigation.
Your doctor may recommend some of the following tests.
General health tests
- Physical examination, including examination of the penis and groin
- Blood and urine tests to check your general health
Biopsy
- A small sample of tissue (called a biopsy) is taken from the affected area of the penis and sometimes also from the lymph nodes (small glands that help filter infection and cancer cells) in your groin. Lymph node biopsies are often guided by ultrasound.
The tissue is examined under a microscope by a pathologist. This test helps confirm whether cancer is present and what type of cancer it is.
Imaging tests
Other imaging tests may be recommended to show how far the cancer has grown or whether it has spread to other parts of the body. These may include:
- Ultrasound
A handheld device (called a transducer) is moved over the penis or the abdomen (tummy). High frequency sound waves create images of the inside of the body and can help doctors look at the penis and assess nearby lymph nodes in the groin. - MRI (magnetic resonance imaging) scan
Uses a strong magnet and radio waves to produce detailed cross sectional images of the penis and nearby structures. A dye injected into a vein may be used to help show abnormal areas more clearly. You may also be given a medicine by injection into the penis to help produce an erection. This helps doctors get clearer images of the area. - CT (computed tomography) scan
Uses X rays and a computer to create detailed images of the lymph nodes, and other parts of the body to check if the cancer has spread. A dye injected into a vein may be used to help highlight abnormal areas. - PET (positron emission tomography)-CT scan
A scan that uses a small amount of radioactive liquid to highlight areas of increased activity in the body, which may indicate cancer. PET scans are not routinely used in penile cancer but may be recommended in selected cases.
The results of these tests help doctors understand how far the penile cancer has spread in the body (this is called the stage) and how abnormal the cancer cells look under the microscope and how likely they are to grow or spread (the grade). This information helps guide decisions about the most appropriate treatment.
Doctors may use the TNM staging system to describe the cancer stage:
- T (Tumour) – size of the tumour and how far it has grown (Ta, Tis, T0–T4)
- N (Nodes) – whether the cancer has spread to nearby lymph nodes
- N0: no spread to lymph nodes
- N1-N3: spread to nearby lymph nodes
- M (Metastasis) – whether the cancer has spread to distant parts of the body
- M0: no distant spread
- M1: distant spread present
The TNM results are often put together to give an overall stage of penile cancer, ranging from Stage 0 (earliest stage) to Stage IV (most advanced stage).
Grading penile cancer
Grading is done by examining cancer cells under a microscope, usually from a biopsy or after surgery. The grade describes how abnormal the cancer cells look compared with normal cells. It gives an idea of how quickly the cancer may grow.
- Low grade cancers: the cancer cells look similar to normal cells and are usually slow-growing
- High grade cancers: the cancer cells look very abnormal and tend to grow more rapidly.
Penile cancer and its treatment can affect physical, sexual, and emotional wellbeing, so care focuses on both treating the cancer and supporting quality of life.
If penile cancer is diagnosed, your doctor may discuss your case with other health professionals at a multidisciplinary team (MDT) meeting. This team may include urologists, medical oncologists, radiation oncologists, nurses, and allied health professionals such as physiotherapists. The MDT works together to recommend the most appropriate treatment options for you.
Treatment recommendations for penile cancer depend on several factors, including:
- the type and extent of penile cancer (including tumour size, grade, and stage)
- whether the cancer has spread
- your overall health, and
- your preferences
It is important to take time to discuss your treatment options, including possible benefits and side effects, with your doctor before deciding which treatment is right for you.
Treatment may include one or more of the following options:
Surgery
Surgery is the main treatment for penile cancer. It involves removing the tumour along with a small amount of surrounding healthy tissue (called a margin).
The type of surgery depends on the size and location of the cancer. In many cases, reconstructive surgery can be used to help preserve the appearance and function of the penis, particularly when the cancer is diagnosed early. Your surgeon will discuss the most suitable surgical approach with you.
If needed, further surgery may also be recommended to remove lymph nodes (small glands that help filter infection and cancer cells) in the groin, and sometimes deeper in the pelvis.
Local treatments
Some early or superficial low-grade penile cancers may be treated with techniques other than surgery.
These may include:
- Laser treatment uses a focused beam of light to destroy cancer cells. One type, called carbon dioxide (CO₂) laser ablation, removes very shallow tissue and is usually used for small, early stage cancers on the surface of the penis.
- Topical chemotherapy, where chemotherapy medicine is applied directly to the affected area as a cream.
Radiation therapy (radiotherapy)
Radiation therapy uses high energy radiation to damage or kill cancer cells. It may be used as the main treatment in some cases, or after surgery.
Radiation therapy is most commonly given as external beam radiation therapy, where the radiation is delivered by a machine outside the body. In some situations, radiation may be given by placing radioactive material into or close to the tumour (called brachytherapy).
Chemotherapy
Chemotherapy uses drugs to damage or kill rapidly dividing cells, such as cancer cells.
- Neoadjuvant chemotherapy
Neoadjuvant chemotherapy is chemotherapy given before surgery. It may help shrink the tumour to make surgery easier and treat cancer cells that may have spread elsewhere in the body, even if they cannot be seen on scans. - Advanced or metastatic disease
Chemotherapy may also be used to treat penile cancer that has spread to other parts of the body (advanced or metastatic cancer).
Chemotherapy for penile cancer is usually given as a combination of drugs through a drip into a vein (intravenously).
Clinical trials
For general information about clinical trials, please click here: What is a clinical trial?
For information about ANZUP penile cancer trials click here: Penile Cancer Trials
All treatments can have side effects, which vary from person to person. Your doctor will discuss the possible benefits and risks with you.
Complementary and alternative therapies
- Complementary therapies
Complementary therapies are used alongside conventional medical treatment and may help manage symptoms or side effects of cancer or its treatment. These may include massage, psychological or relaxation techniques, and some herbal or natural therapies. - Alternative therapies
Alternative therapies are used instead of conventional medical treatment. Most have not been scientifically tested for safety or effectiveness, and some therapies may interfere with cancer treatments or cause harm.
It is important to tell your cancer doctor about any complementary or alternative therapies you are using or considering before starting or during cancer treatment.